










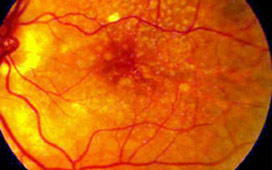
Diabetes is a disease, which affects the small blood vessels of all the organs of the body. As the disease progresses it inevitably involves the microvascular architecture i.e. the blood supply of the retina (sensory part of the eye) also. This manifestation of diabetes is called as diabetic retinopathy. To simplify – It is a disease of the blood vessels of the retina due to diabetes.
Diabetes is a disease, which affects the small blood vessels of all the organs of the body. As the disease progresses it inevitably involves the microvascular architecture i.e. the blood supply of the retina (sensory part of the eye) also. This manifestation of diabetes is called as diabetic retinopathy.
To simplify – It is a disease of the blood vessels of the retina due to diabetes.
The main cause is long standing diabetes.
• Among younger-onset patients with diabetes (Type 1), upto 8% of individuals will have this disease after 3 years of diagnosis and 25% at 5 years, 60% at 10 years, and 80% of diabetics will have this eye problem by 15 years.
• In older type 2 diabetics up to 21% of patients have diabetic retinopathy at the time of first diagnosis of diabetes, and most develop some degree of retinopathy over time. Uncontrolled diabetes , High blood pressure, High cholesterol, Kidney disease and Low Haemoglobin worsen diabetic retinopathy.
It may be asymptomatic for a long time.
Once the macula , i.e. the central part of the retina develops swelling , there would be a deterioration in eyesight.
If there is bleeding within and in front of the retina, floaters would be seen or the vision may be drastically reduced. Floaters is seeing black spots or lines moving in front of the eye.
Once the central retina is detached the vision loss becomes severe and chances of recovery even after surgery become less.
It can be diagnosed by a simple dilated eye examination to see the retina in detail. If significant changes are found then investigations like Fluorescein Angiography and Optical Coherence Tomography may be done.
Fluorescein Angiography involves taking photographs of the retina after injecting a dye in a vein in the patient's arm. The dye reaching the eye helps to clarify the type and extent of disease, including detail of abnormal vessels and leakage.
Optical Coherence Tomography : In this test images of the retina are taken to show its microscopic detail.
The gold standard of therapy is Retinal LASER Photocoagulation. LASER can help to prevent a bleed in the eye and also decrease swelling of the retina. However, it cannot usually restore vision lost due to the retinal damage. It has to be appropriately timed. The Lasers used for this purpose are Green & Red Diode Laser. Other options now available are injecting drugs like steroids and AVASTIN into the eye. These drugs also aim to reduce the swelling in the retina and help in drying up of the abnormal blood vessels. These are quite effective and can even improve vision in some cases. A major drawback is the effect of these drugs is time limited and many patients require re-injections. Combination therapy of LASER and injections is also being done.
Advanced cases with non-resolving bleed (Vitreous Hemorrhage) in the eye or retinal detachment require advanced microsurgery. This involves highly complex Vitreo-Retinal surgical procedures. Today with highly advanced technology, some amount of visual recovery can be achieved in a large number of advanced cases also.
Cases which present early and are adequately lasered generally maintain good vision. A good control of diabetes is most important to slow the progression of disease. A combination of injectable drugs and laser has improved the outcome in moderately advanced cases also. The outcome may not be very good in advanced cases even after surgery, however still some useful vision can be retained.
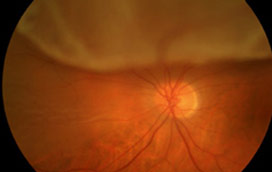
Age Related Macular Degeneration (ARMD) is degeneration of the most sensitive part of the retina (sensory part of the eye) called macula. It is mostly seen in people over the age of 50 years. Initially it is a silent disease and can affect one eye to begin with. At this stage it might be detected by an ophthalmologist on routine retina evaluation. Gradually vision loss increases mainly in the center allowing vision at sides, but makes reading or close work difficult without the use of special low vision aids. The early stages of ARMD typically start with appearance of deposits beneath the retina called Drusen. These do not affect vision very much by themselves and most people with Drusen will never have a serious loss of vision. However, certain changes may occur that lead to the late stage of ARMD which leads to marked visual loss.
The exact cause of macular degeneration is not known though following risk factors have been identified: age, heredity, sex (women more affected then men), light ocular pigmentation, hypertension, cardiovascular diseases, diabetes, photo toxicity and cigarette smoking.
Types: There are 2 types of ARMD: "Dry" and "Wet"
Dry ARMD is the most common form accounting 80-90% of all cases and is associated with ageing. It is caused by degeneration in visual cells leading to yellow-white deposits in layers of retina called drusen or formation of atrophic areas in macula. Overtime dry ARMD may develop into wet type.
Wet or Exudative ARMD is the more severe variety where abnormal blood vessels form beneath the macula which leak fluid and blood under the retina. Blood under the retina is toxic to the photoreceptors and can lead to severe loss of function of retina
If only one eye is affected to begin with, the symptoms may not be noticeable in early stages. Gradually as disease progresses or if both eyes are involved, reading or close work may become difficult. Common symptoms are distortion of objects which are looked at directly, for e.g. bulges or curved appearance of a straight door, distorted print lines in book (metamorphopsiae), missing of letters or words while reading, a dark or blank spot in the center of vision, (scotoma) or fading of colors specially blue (dyschromatopsiae)
As initially it is a silent disease, mostly it is picked up in a routine retina examination by an ophthalmologist .The retinal examination done by an ophthalmoscope will show the findings of this disease process. To assess the condition in detail, certain other test are done:
Amsler Grid: It is a test paper with graphic picture to be used at reading distance with near glasses on. This is used to check for extent of sight loss-dark spot, distortion or missing of straight lines and also is given to the patient to take home so that he can monitor his symptoms at home and report immediately if there is worsening.
Fundus Fluorescin Angiography (FFA) / Indocyanine Green Angiography (ICG): the photographs of macula are taken after injecting a dye in patient's arm. The dye reaching the eye helps to clarify the type and extent of disease, including detail of abnormal vessels, leaks and membrane formations.
Optical Coherence Tomography (OCT) : In this test photographs of the retina are taken to show its microscopic detail. So it can help detect any early thickening of the retina in wet ARMD. Also it can delineate the abnormal blood vessels ( choroidal neovascularisation ) from where the blood oozes. Changes of dry ARMD such as drusen can also be demonstrated. Also it is an excellent tool to follow up after treatment to assess the effect of the treatment done and need for re-treatment.
There is no prevention of ARMD. Early detection is the key to prevent severe loss of vision. All individuals above 50,especially if there is a family history of ARMD, history of cardiovascular disease, light ocular pigmentation, should get annual retinal check up for the same. Anyone experiencing following symptoms should consult an ophthalmologist immediately:
Straight lines appearing distorted-specially in the center of vision
Dark blurry or white patch in the center of vision
Color perception changes
Smoking is a risk factor and should be avoided at all costs if any of the risk factor is present.
According to some recent international multicentric trials, multivitamins may slow down progression of dry ARMD. However, excess of fat soluble multivitamins can have their own side-effects and thus consult your doctor before regularly taking multivitamin pills.
There is no permanent cure for dry ARMD. The aim of management is to keep a vigilant check on progression of disease and take measures to improve functional capability of the patient.
The mainstay of treatment of wet ARMD at present is injection of Anti-VEGF drugs into the eye. These are special molecules designed to stop further development of blood vessels. So once the abnormal vessel growth under the retina gets inhibited the leakage of fluid and blood also reduces. However at present these injections need to be repeated at regular intervals as once the effect of the drug wanes off the abnormal vessels star growing again. The two main such drugs being used at present are AVASTIN & LUCENTIS. Presently we donot have a drug which can altogether end the process of this abnormal neovascularisation. A lot of research is ongoing to find a permanent cure for ARMD.
Other treatment modalities available for wet ARMD are -

A macular hole is a small break in the macula, located in the center of the eye's light-sensitive tissue called the retina.
The eye contains a jelly-like substance called the vitreous. Shrinking of the vitreous usually causes the hole. As a person ages, the vitreous becomes watery and begins to pull away from the retina. If the vitreous is firmly attached to the retina when it pulls away, a hole can result.Macular holes are related to aging and usually occur in people over age 60.Macular holes can also occur in other eye disorders, such as high myopia (nearsightedness), injury to the eye, retinal detachment, and, rarely, macular pucker. As a person ages, the vitreous becomes watery and begins to pull away from the retina. If the vitreous is firmly attached to the retina when it pulls away, a hole can result.
Macular holes often begin gradually. In the early stage of a macular hole, people may notice a slight distortion or blurriness in their straight-ahead vision. Straight lines or objects can begin to look bent or wavy. Reading and performing other routine tasks with the affected eye become difficult.
During an eye exam, the ophthalmologist will dilate eye pupils and examine the retina. The other test test called fluorescein angiography that uses dye to illuminate areas of the retina can also be done for diagnosis of hole. Another test called optical coherence tomography (OCT) is most helpful in making an accurate macular hole diagnosis. With OCT, a special diagnostic laser camera is used to photograph your retina. It measures the thickness of the retina and is also very sensitive at detecting swelling and fluid. OCT can also diagnose small macular holes that are too small to be seen in an examination or with angiography.
Although some macular holes can seal themselves and require no treatment, surgery is necessary in many cases to help improve vision. In this surgical procedure-- called a vitrectomy-the vitreous gel is removed to prevent it from pulling on the retina and replaced with a bubble containing a mixture of air and gas. The bubble acts as an internal, temporary bandage that holds the edge of the macular hole in place as it heals. Surgery is performed under local anesthesia and often on an out-patient basis. Following surgery, patients must remain in a face-down position, normally for a day or two but sometimes for as long as two-to-three weeks. This position allows the bubble to press against the macula and be gradually reabsorbed by the eye, sealing the hole. As the bubble is reabsorbed, the vitreous cavity refills with natural eye fluids. Maintaining a face-down position is crucial to the success of the surgery. Because this position can be difficult for many people, it is important to discuss this with the doctor before surgery.
Retina is the neural layer at the back of the eye that transforms luminous energy of the image received by the eye to neural energy transmitted ahead to the brain. In terms of a very common comparison, the eye being the camera the retina is the film. However, the film gets exposed to light and the image is recorded on it… the retina is a dynamic structure that needs nourishment and consumes energy.
Movement of retina from its usual location is called retinal detachment. It usually signifies the separation of the pigment layer from the sensory layer. This cuts the retina off from its blood supply and nutrition. The retina will degenerate and lose its ability to function if it stays detached long enough.
The retina may tear at certain points due to pull by the vitreous gel. A child's vitreous has the consistency of egg white… and is firmly attached to the retina at certain points. Usually with changes in hydration of the vitreous, it separates from the underlying retina. This separation usually is trouble and symptom free… but may cause ters in the retina at times. This allows fluid to seep under and elevates the retina from the choroid ( The pigment and vessel layer that nourishes the retina)
The most sensitive area of the retina is the Macula. This is primarily composed of cones and is responsible for the fine visual work we put our eyes to – reding, recognizing faces etc. The peripheral retina is primarily composed of rods.
There are three major types of retinal detachment:
Rhegmatogenous (Break)
A break in the sensory layer can cause the fluid to seep in and lifts the retina off. This is more commonly seen in eyes weakened by HIGH MYOPIA, EYE INJURY or PREVIOUS EYE SURGERY
Traction
This is the kind of detachment that develops when strands of vitreous or scar tissue pull on the retina as happens in DM
Exudative
This kind of detachment results when any inflammatory disease of the eye results in collection of fluid under the retina due to swelling or bleeding
Each of these would need a different approach and comprehensive care facility to treat the patient as a whole and not an isolated episode of sight threat.
All rhegmatogenous retinal detachments need immediate specialist consult atleast. All fresh RDs MUST be treated surgically within 24-48 hours. All chronic and longstanding RDs must be addressed within a week of diagnosis.
Exudative Rds usually resolve spontaneously with appropriate menegement of the underlying condition.
Traction RDs require pars plana vitrectomy and silicone oil tamponade.
Small tears or breaks may be managed by LASER photocoagulation or cryopexy.
True RDs require surgical intervention. This may be in the form of